What Causes Alzheimer’s? Scientists Are Rethinking the Answer.
Scientists have long held onto the idea that sticky blobs of proteins sitting between brain cells are the cause of Alzheimer’s disease. Now, however, many are turning their attention to deeper dysfunctions happening within cells.
Harol Bustos for Quanta Magazine
Introduction
It’s often subtle at first. A lost phone. A forgotten word. A missed appointment. By the time a person walks into a doctor’s office, worried about signs of forgetfulness or failing cognition, the changes to their brain have been long underway — changes that we don’t yet know how to stop or reverse. Alzheimer’s disease, the most common form of dementia, has no cure.
“There’s not much you can do. There are no effective treatments. There’s no medicine,” said Riddhi Patira, a behavioral neurologist in Pennsylvania who specializes in neurodegenerative diseases.
That’s not how the story was supposed to go.
Three decades ago, scientists thought they had cracked the medical mystery of what causes Alzheimer’s disease with an idea known as the amyloid cascade hypothesis. It accused a protein called amyloid-beta of forming sticky, toxic plaques between neurons, killing them and triggering a series of events that made the brain waste away.
The amyloid cascade hypothesis was simple and “seductively compelling,” said Scott Small, the director of the Alzheimer’s Disease Research Center at Columbia University. And the idea of aiming drugs at the amyloid plaques to stop or prevent the progression of the disease took the field by storm.
Decades of work and billions of dollars went into funding clinical trials of dozens of drug compounds that targeted amyloid plaques. Yet almost none of the trials showed meaningful benefits to patients with the disease.
That is, until September, when the pharmaceutical giants Biogen and Eisai announced that in a phase 3 clinical trial, patients taking the anti-amyloid drug lecanemab showed 27% less decline in their cognitive health than patients taking a placebo did. Last week, the companies revealed the data, now published in the New England Journal of Medicine, to an excited audience at a meeting in San Francisco.
Because Alzheimer’s disease progresses over 25 years, the hope is that lecanemab, when given to people with early-stage Alzheimer’s disease, will slow that progression, said Paul Aisen, a professor of neurology at the Keck School of Medicine of the University of Southern California. By extending the milder stages of the disease, the drug could give people more years of independence and more time to manage their finances before being institutionalized. “To me, that’s really important,” he said.
Some are less hopeful that the results will show any meaningful difference. “It’s nothing different [from] what we saw in the earlier trials,” Patira said.
“The clinically important difference is probably not there,” said Eric Larson, a professor of medicine at the University of Washington. On the scale the companies used to test the efficacy — calculated from interviews with the patient and their caregivers on their memory, judgment and other cognitive functions — their results were statistically significant but modest. And statistical significance, which means the results were likely not due to chance, does not always equate to clinical significance, Larson said. The difference in the rate of decline, for example, might be unnoticeable to caregivers.
What’s more, reports of brain swelling in some participants and two deaths — which the companies deny are due to the drug — has some concerned about the safety of the drug. But Alzheimer’s medicine is a field more accustomed to disappointment than success, and even the announcement by Roche that a second much-awaited drug, gantenerumab, failed in phase 3 clinical trials didn’t diminish the excitement over the lecanemab news.
Do these results mean the amyloid cascade hypothesis was right?
Not necessarily. It does suggest to some researchers that with more coaxing, targeting amyloid could still lead to effective therapeutics. “I’m thrilled,” said Rudy Tanzi, an investigator at Massachusetts General Hospital. Lecanemab doesn’t offer a “stellar effect,” he acknowledged, but it’s a “proof of concept” that could potentially lead to more effective drugs or more effectiveness if taken earlier.
Many researchers, however, aren’t convinced. To them, the small to nonexistent effect sizes in these trials and earlier ones suggest that amyloid plaques are not the cause of the disease. Amyloid is “more the smoke, not the fire … which continues to rage inside neurons,” said Small.
Not Dead but Insufficient
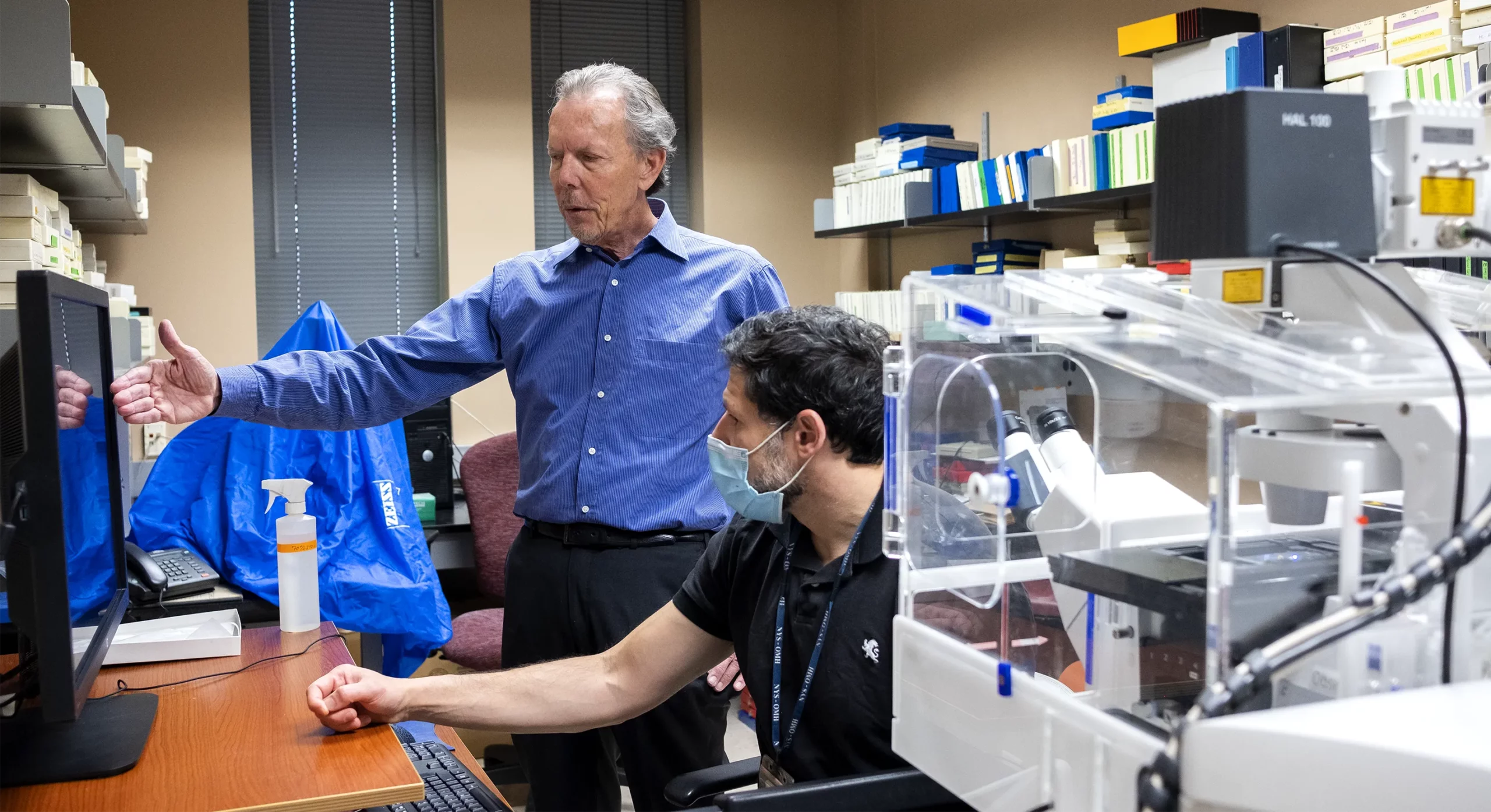
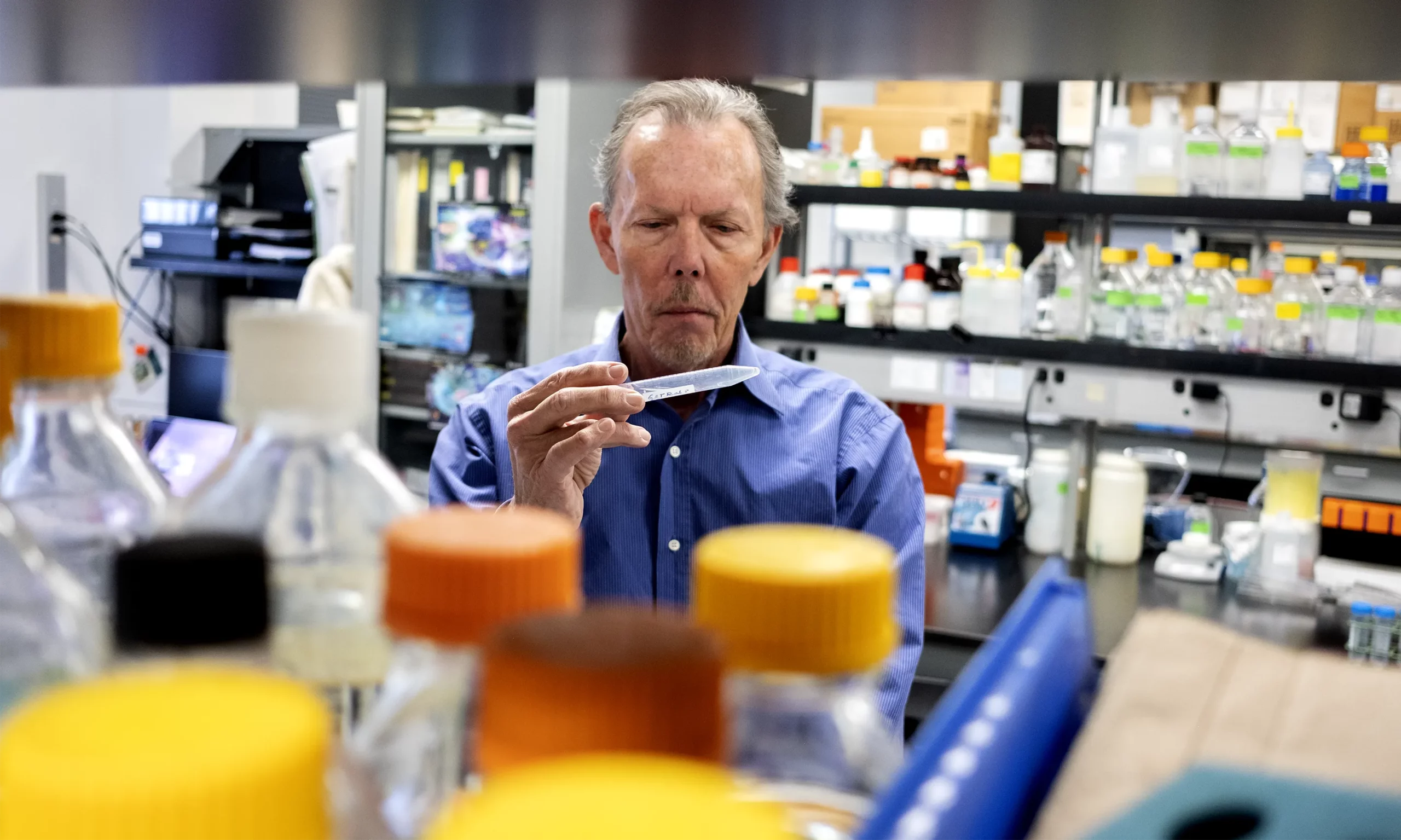
The underwhelming effects of lecanemab neither surprised nor impressed Ralph Nixon, the director of research at the Center for Dementia Research at the Nathan S. Kline Institute for Psychiatric Research in New York. “If that was your goal, to reach this point in order to claim victory of that hypothesis, then you’re using the lowest possible bar I can think of,” he said.
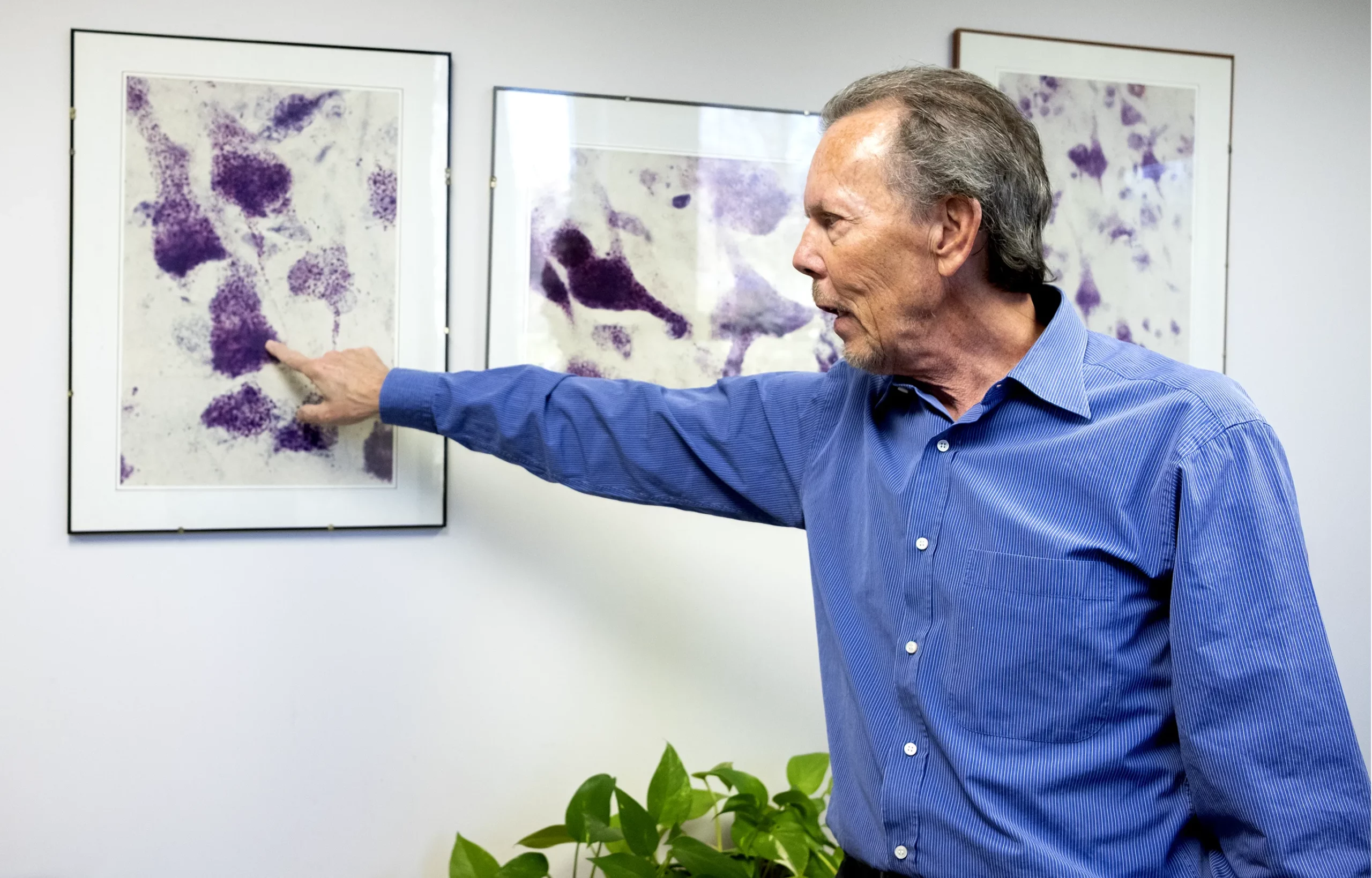
The researcher Ralph Nixon points to an abnormal blob amid the brain tissue of an Alzheimer’s patient in a microscopy image taken in the 1990s.
Karen Dias for Quanta Magazine
Nixon has worked in the trenches of Alzheimer’s disease research since the earliest days of the amyloid cascade hypothesis. But he has been a leader in exploring an alternative model for what causes the disease’s dementia — one of many other possible models that were largely ignored in favor of the amyloid explanation despite its lack of useful results, according to many researchers.
A stream of recent findings has made it clear that other mechanisms may be at least as important as the amyloid cascade as causes of Alzheimer’s disease. To say that the amyloid hypothesis is dead would be overstating it, said Donald Weaver, a co-director of the Krembil Brain Institute in Toronto, but “I would say that the amyloid hypothesis is insufficient.”
The emerging new models of the disease are more complex than the amyloid explanation, and because they are still taking shape, it’s not clear yet how some of them may eventually translate into therapies. But because they focus on fundamental mechanisms affecting the health of cells, what’s being learned about them might someday pay off in new treatments for a wide variety of medical problems, possibly including some key effects of aging.
Many in the field, including some who still stand behind the amyloid cascade hypothesis, agree that there’s a more complex story taking place in the folds of the brain. While these alternate ideas were once hushed and thrown under the rug, now the field has broadened its attention.
On the wall of Nixon’s office hangs a set of framed microscopy photos, images from an Alzheimer’s patient’s brain that were snapped almost 30 years ago in his lab. Nixon points to a bulky purple blob in the photos.
“We saw the same things that we saw recently … back in the 1990s,” Nixon said. But because of preconceptions about amyloid plaques, he and his colleagues couldn’t recognize the blobs for what they really were. Even if they had, and if they had told anyone, “we would have been run out of the field back then,” he said. “I was able to survive long enough to now have people believe.”
The Suspicious Plaques
Scientists studying Alzheimer’s disease often bring a deep passion to their work, not just because it’s addressing a major health burden, but because it’s one that often strikes close to home. That’s certainly the case for Kyle Travaglini, an Alzheimer’s researcher at the Allen Institute for Brain Science in Seattle.
On a hot August day in 2011, when Travaglini was starting his freshman year at the University of California, Los Angeles, he welcomed his grandparents for a college visit. As a boy, he had spent many happy hours walking with his grandmother in San Diego’s Japanese Friendship Garden, so it seemed only right that they should tour the UCLA campus together.

By the time the researcher Kyle Travaglini graduated from the University of California, Los Angeles in 2015, his grandmother had advanced cognitive decline from Alzheimer’s.
Courtesy of Kyle Travaglini
He and his grandparents strolled among the university’s giant pines and across its vast, open plazas. They peered up at the beautiful brick-and-tile facades of buildings built in the Romanesque style. His beaming grandparents asked him about everything they passed. “What’s this building?” his grandmother would ask.
Then she’d face the same building and ask again. And again.
“That tour was when I first started to notice … something is really kind of wrong,” Travaglini said. In the following years, his grandmother often blamed her forgetfulness on being tired. “I don’t think she ever really wanted us to see it,” he said. “It was a lot of masking.” Eventually, his grandmother was diagnosed with Alzheimer’s disease, just as her own mother and tens of millions of other people around the world have been.
His grandfather initially resisted the idea that she had Alzheimer’s disease, as spouses of patients often do, according to Patira. That denial eventually turned into frustration that there wasn’t anything they could do, Travaglini said.
Old age doesn’t guarantee the development of Alzheimer’s disease — but it’s the greatest risk factor. And as the global average life span increases, Alzheimer’s disease endures as a major public health burden, and one of the greatest unsolved mysteries of modern medicine.
Starting with memory impairment and cognitive decline, the disease eventually affects behavior, speech, orientation and even a person’s ability to move. Because the living human brain is complex and experiments on it are largely impossible, scientists often have to rely on rodent models of the disease that don’t always translate to humans. What’s more, patients with Alzheimer’s disease often have other types of dementias at the same time, which makes it difficult to tease apart what exactly is happening in the brain.
Though we still don’t know what causes Alzheimer’s, our knowledge about the disease has grown dramatically since 1898, when Emil Redlich, a doctor at the Second Psychiatric Clinic of the University of Vienna, first used the word “plaques” to describe what he saw in the brains of two patients diagnosed with “senile dementia.” In 1907 the German psychiatrist Alois Alzheimer described the presence of plaques, tangles and atrophy visualized by a silver staining technique in the brain of Auguste Deter, a woman who had died at the age of 55 from “presenile dementia.” That same year, the Czech psychiatrist Oskar Fischer reported 12 cases of plaques, which he referred to as “drusen” after the German word for a cavity in a rock with an interior lined with crystals.
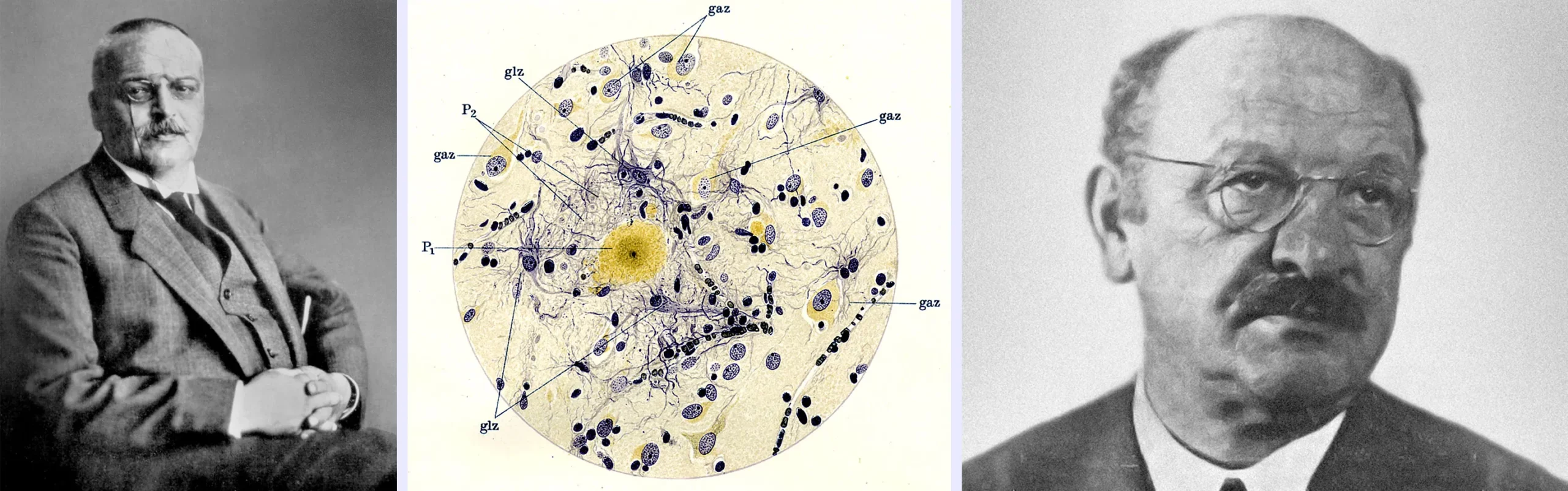
From left: Alois Alzheimer, an illustration by Alzheimer of the plaques appearing in the brains of patients with dementia, and Oskar Fischer.
From left: Science Source; Reprinted from Current Biology, 6/21, Ralf Dahm, Alzheimer’s discovery, 5, Copyright (2006), with permission from Elsevier; Courtesy of Filip em
By 1912, Fischer had identified dozens of dementia patients with plaques, and he had described their cases in unprecedented detail. Yet Emil Kraepelin, a founder of modern psychiatry and Alzheimer’s boss at a psychiatric clinic in Munich, Germany, decreed that the condition was to be named “Alzheimer’s disease.” Fischer and his contributions were lost for decades after he was arrested by the Gestapo in 1941 and taken to a Nazi political prison, where he died.
Over the next several decades, more knowledge about the disease trickled in, but it remained a niche area of interest. Larson recalls that when he was a medical student in the 1970s, Alzheimer’s disease was still mostly ignored by researchers — as was aging in general. It was accepted that when you got old, you stopped being able to remember things.
The “treatments” for these conditions of old age could be harrowing. “People were tied in chairs, and people were given drugs that made them worse,” Larson said. Everyone thought dementia was just a consequence of getting old.
All of that changed in the 1980s, however, when a series of papers established the critical finding that the brains of elderly patients with dementia and the brains of younger patients with presenile dementia looked the same. Physicians and researchers realized that dementia might be not just a consequence of old age but a discrete and potentially treatable disease. Then attention started pouring in. “The field has just been bursting at the seams for decades now,” Larson said.
At first, there were many vague, untestable theories about what might be causing Alzheimer’s disease, ranging from viruses and aluminum exposure to environmental toxins and a nebulous idea called “accelerated aging.” A turning point came in 1984, when George Glenner and Caine Wong at the University of California, San Diego discovered that the plaques in Alzheimer’s disease and the plaques in the brains of people with Down syndrome (the chromosomal disorder trisomy 21) were made of the same amyloid-beta protein. The formation of amyloid plaques in Down syndrome was genetically driven, so might that mean the same was true of Alzheimer’s disease?
Where this amyloid-beta came from was unclear. Maybe it was released by the neurons themselves, or maybe it came from elsewhere in the body and infiltrated the brain through the blood. But suddenly researchers had a likely suspect to blame for the neurodegeneration that ensued.
Glenner and Wong’s paper drew attention to the idea that amyloid might be a root cause of Alzheimer’s. But it took a seminal genetic finding by John Hardy’s laboratory at St. Mary’s Hospital Medical School in London to electrify the research community.
The Curse on Family 23
It began one night in 1987, as Hardy was sifting through a pile of letters on his desk. Because he had been trying to uncover genetic mutations that might lead to Alzheimer’s disease, he and his team had posted an advertisement in an Alzheimer’s Society newsletter, seeking the assistance of families in which more than one individual had developed the disease. The letters had arrived in response. Hardy began reading from the top of the stack, but the first letter the team had received — the one that changed everything — was at the bottom.
“I … think my family could be of use,” read the letter from Carol Jennings, a schoolteacher in Nottingham. Jennings’ father and several of her aunts and uncles had all been diagnosed with Alzheimer’s disease in their mid-50s. The researchers sent a nurse to collect blood samples from Jennings and her kin, whom Hardy anonymized in his work as Family 23 (because Jennings’ letter was the 23rd that he read). Over the next few years, they sequenced the family’s genes, searching for a shared mutation that could be the Rosetta stone for understanding the condition.
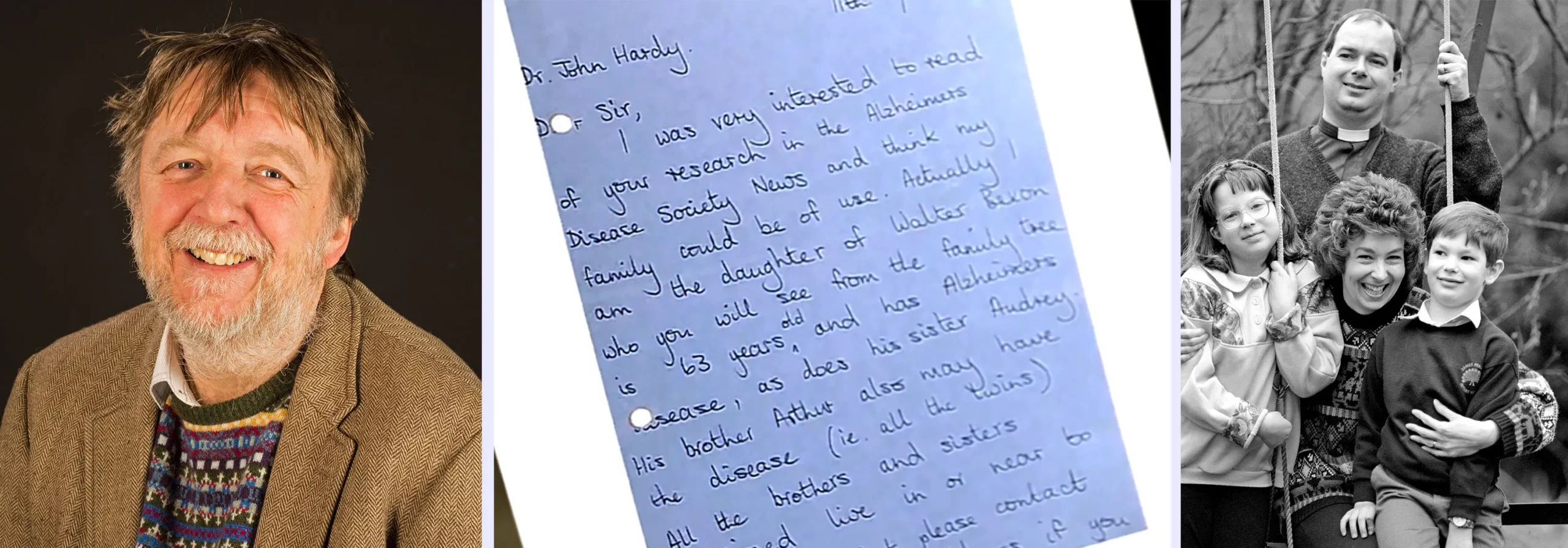
The letter that Carol Jennings wrote in 1986 to the researcher John Hardy, pictured at left, led to the pivotal discovery that a single mutation caused her family’s inherited early-onset form of Alzheimer’s. At right is a photo, taken in 1992, of Carol Jennings, her husband Stuart and their two children.
From left: Courtesy of UCL QS IoN Medical Illustration; Courtesy of the BBC and Stuart Jennings; Ross Kinnaird/PA Images/Alamy Stock Photo
On November 20, 1990, Hardy and his teammates stood in the office of their lab, listening to their colleague Marie-Christine Chartier-Harlin describe the latest results of her genetic sequencing. “As soon as she found the mutation, we knew what it meant,” Hardy said. Jennings’ family had a mutation in the gene for the amyloid precursor protein (APP), which researchers had isolated for the first time only a few years before. As its name suggests, APP is the molecule that enzymes break apart to form amyloid-beta; the mutation caused an overproduction of the amyloid.
Hardy hurried home that day, and he remembers telling his wife, who was breastfeeding their first child as she listened to his news, that what they’d just found “was going to change our lives.”
A few months later, around Christmas, Hardy and his team organized a conference at the geriatric clinic in a hospital in Nottingham to present their findings to Jennings and her family. There was one sister, Hardy remembers, who kept saying, “Thank goodness, it’s missed me.” But it was obvious to Hardy after spending a bit of time with her that it hadn’t; everyone else in the family already knew that she had the disease as well.
Jennings’ family was mildly religious, Hardy said. They kept saying that maybe they were chosen to help in the research. They were distressed but proud of what they had contributed — as they should be, Hardy said.
The following February, Hardy and his team published their results in Nature, cluing in the world to the APP mutation and its significance. The form of Alzheimer’s disease that the Jennings family has is rare, affecting only around 600 families worldwide. People with a parent who carries the mutation have a 50% chance of inheriting it and developing the condition — if they do, it’s almost certain that they will develop it before the age of 65.
No one knew how far the similarities might go between the Jennings’ kind of inherited Alzheimer’s disease and the much more common late-onset form that typically occurs after the age of 65. Still, the discovery was suggestive.
The following year, over a long weekend, Hardy and his colleague Gerald Higgins typed up a landmark perspective that used the term “amyloid cascade hypothesis” for the first time. “I wrote what I thought was a simple article saying, basically, if amyloid causes the disease in this case, maybe amyloid is the cause in all cases,” Hardy said. “I just typed it, sent it off to Science and they took it without any changes.” He didn’t foresee how popular it would become: It has now been cited over 10,000 times. It and an earlier review published by Dennis Selkoe, a researcher at Harvard Medical School and Brigham and Women’s Hospital in Boston, became foundational documents for the new amyloid cascade hypothesis.
Looking back on those early days, “I thought that anti-amyloid therapies would be like a magic bullet,” Hardy said. “I certainly don’t think that now. I don’t think anybody thinks that.”
Leaky Bags of Acid
Researchers soon started flocking to the beauty and simplicity of the amyloid cascade hypothesis, and a collective goal of targeting the plaques and getting rid of them as a remedy for Alzheimer’s started to emerge.
In the early 1990s, the field became “monolithic in its thinking,” said Nixon. But he and some others were unconvinced. The idea that amyloid killed neurons only after it was secreted and formed deposits between the cells made less sense to him than the possibility that the amyloid accumulated inside neurons and killed them before it was released.

After the amyloid cascade hypothesis was proposed, the field of Alzheimer’s research became “monolithic in its thinking,” said Nixon.
Karen Dias for Quanta Magazine
Nixon was following the thread of a different theory at Harvard Medical School. At the time, Harvard had one of the very first brain banks in the nation. When anyone died and donated their brain to science, it was cut into slices and frozen at minus 80 degrees Celsius for later examination. “It was a huge operation,” Nixon said, and one that made Harvard a hub for Alzheimer’s research.
One day, Nixon switched on a microscope and aimed it at a slice of brain stained with antibodies against certain enzymes. Through the microscope’s light he could see that the antibodies were congregating on plaques outside the cells. It was immensely surprising: The enzymes in question were usually only seen in the organelles called lysosomes. “That suggested to us that the lysosome was abnormal and was leaking out these enzymes,” Nixon said.
The Belgian biochemist Christian de Duve, who discovered lysosomes in the 1950s, sometimes referred to them as “suicide bags” because they are instrumental in a vital (but at the time poorly understood) process called autophagy (“self-eating”). Lysosomes are membrane vesicles holding an acidic slurry of enzymes that break apart obsolete molecules, organelles, and anything else the cell doesn’t need anymore, including potentially harmful misfolded proteins and pathogens. Autophagy is an essential process, but it’s especially critical for neurons because unlike nearly all the other cells in the body, mature neurons do not divide and replace themselves. They must be able to survive for a lifetime.
Were parts of the adjacent neurons degenerating and leaking the enzymes? Were the neurons falling apart entirely? Whatever was happening, it hinted that the plaques were not simply products of amyloid accumulating in the space between neurons and killing them. Something might be going wrong inside the neurons themselves, maybe even before the plaques formed.
But Selkoe and other colleagues at Harvard didn’t share Nixon’s enthusiasm about the lysosomal findings. They weren’t hostile to the idea, and they all stayed collegial. Nixon even served on the thesis committee for Tanzi, who had named the APP gene and been one of the first to isolate it, and who had become an ardent advocate for the amyloid cascade hypothesis.
“All of these people were friends. … We just had different views,” Nixon said. He recalls that they were congratulatory about work well done but with an undertone, he said, of “we don’t personally think it’s as relevant to Alzheimer’s as the amyloid-beta story. And we don’t frankly care.”
No Alternatives Allowed
Nixon was hardly the only one nurturing alternatives to the amyloid cascade hypothesis. Some researchers thought that the answer might lie in the tau tangles — abnormal bundles of proteins inside neurons that are also hallmarks of Alzheimer’s disease and even more closely linked to the cognitive symptoms than amyloid plaques are. Others thought that excessive or misplaced immune activity might be inflaming and damaging delicate neural tissue. Still others began suspecting dysfunctions in cholesterol metabolism or in the mitochondria that power neurons.
But notwithstanding the range of alternative theories, by the end of the 1990s, the amyloid cascade hypothesis was the clear darling of the biomedical research establishment. Funding agencies and pharmaceutical companies were beginning to pour billions into the development of anti-amyloid treatments and clinical trials. At least in terms of relative funding, the alternatives were swept under the carpet.


Merrill Sherman/Quanta Magazine
It’s worth considering why. Although major elements of the amyloid hypothesis were still a cipher, such as where the amyloid came from and how it killed neurons, the idea was in some ways gloriously specific. It pointed to a molecule; it pointed to a gene; it pointed to a strategy: Get rid of these plaques to stop the disease. To everyone desperate to end the misery of the Alzheimer’s scourge, it at least offered a plan of action.
In contrast, other theories were still relatively shapeless (in no small part because they hadn’t gotten as much attention). Faced with the choice of either chasing cures based on amyloid or pursuing a nebulous something-more-than-amyloid, the medical and pharmaceutical communities made what seemed like the rational choice.
“There was a kind of Darwinian competition of ideas about which ones are going to be tested,” Hardy said, “and the amyloid hypothesis won.”
Between 2002 and 2012, 48% of the Alzheimer’s drugs under development and 65.6% of the clinical trials were focused on amyloid-beta. A mere 9% of the drugs were aimed at tau tangles, the only targets other than amyloid that were considered potential causes of the disease. All the rest of the drug candidates aimed to protect neurons from degeneration to cushion against the effects of the disease after it started. Alternatives to the amyloid cascade hypothesis were scarcely in the picture.
If only the amyloid-focused drugs had worked.
In his laboratory at the Nathan S. Kline Institute for Psychiatric Research, Nixon and his colleague Philip Stavrides look at microscopy images of Alzheimer’s brain tissue.
Karen Dias for Quanta Magazine
Drugs and Dashed Hopes
It didn’t take long for disappointing results to start rolling in from the drug trials and experimental tests of the amyloid hypothesis. In 1999, the pharmaceutical company Elan created a vaccine that was meant to train the immune system to attack amyloid protein. The company stopped the trial in 2002, however, because some patients receiving the vaccine developed dangerous brain inflammation.
In the following years, several companies tested the effects of synthetic antibodies against amyloid and found that they caused no changes in cognition in the Alzheimer’s patients receiving them. Other drug trials took aim at the enzymes that cleaved amyloid-beta from the parent APP protein, and some tried to clear out existing plaques in patients’ brains. None of these worked as hoped.
By 2017, 146 drug candidates for treating Alzheimer’s disease had been deemed unsuccessful. Only four drugs had been approved, and they treated the symptoms of the disease, not its underlying pathology. The results were so disappointing that in 2018, Pfizer pulled out of Alzheimer’s research.
A 2021 review that compared the results of 14 of the major trials confirmed that reducing extracellular amyloid did not greatly improve cognition. There were also failures in trials that focused on targets other than amyloid, like inflammation and cholesterol, though there were far fewer trials for these alternatives, and thus far fewer failures.
“It was just so dismal,” said Jessica Young, an associate professor at the University of Washington. As she went through school, first pursuing cell biology, then neurobiology, and finally Alzheimer’s research specifically, she watched as clinical trial after clinical trial failed. It was “disheartening to younger scientists who really wanted to try to make a difference,” she said. “Like, how do we get over this? It’s not working.”
There was one brief bright spot, however. In 2016 an early trial of aducanumab, a drug developed by Biogen, showed promise for reducing amyloid plaques and slowing the cognitive decline of Alzheimer’s patients, the authors reported in Nature.
But in 2019 Biogen shut down their phase 3 clinical trial, saying that aducanumab didn’t work. The following year, after reanalyzing the data and concluding that aducanumab did work in one of the trials after all — modestly, in a subset of patients — Biogen requested approval for the drug from the Food and Drug Administration.
The FDA approved aducanumab in 2021 over the objections of its scientific advisers, who argued that its benefits seemed too marginal to outweigh its risks. Even several researchers who were loyal to the amyloid hypothesis were infuriated by the decision. Medicare decided not to cover the cost of the drug, so the only people taking aducanumab are in clinical trials or able to pay for it out of pocket. After three decades of global research primarily centered on the amyloid hypothesis, aducanumab is the only approved drug that aims at the underlying neurobiology to slow the progression of the disease.
“You can have the most beautiful hypothesis, but if it doesn’t play out with therapeutic efficacy, then it’s not worth anything,” Nixon said.
‘Just One More Experiment’
Of course, the failures of clinical trials don’t necessarily mean that the science they are based on is invalid. In fact, amyloid-hypothesis supporters have often argued that many of the attempted therapies could have failed because patients enrolled in the trials didn’t get the anti-amyloid drugs early enough in the progression of their disease.
The problem with that defense is that since no one knows for certain what causes Alzheimer’s disease, there’s no way of knowing how early the interventions need to be. Risk factors might arise when you’re 50 years old, or when you’re 15. If they happen very early in life, are they definitive causes of a condition that occurs decades later? And how useful can a potential treatment be if it needs to be prescribed that early?
“The amyloid hypothesis has evolved over time so that every time there’s a new set of findings that questions some aspect of it, it morphs into a different hypothesis,” Nixon said. But the fundamental premise, that extracellular amyloid plaques are the trigger for all the other pathologies, has stayed the same.
To Small, a researcher who works on alternate theories, a few of the amyloid cascade supporters who continue to hold their breath for encouraging results have “moved from being dispassionate scientists to being a little bit more ideological and religious,” he said. “They’re in this sort of self-fulfilling world of always ‘just one more experiment.’ It doesn’t make scientific sense.”
Moreover, Small notes that while the drug trials were floundering, new scientific findings were poking holes in the fundamental hypothesis as well. Neuroimaging studies, for example, were confirming previous autopsy findings that some people who died with extensive amyloid deposits in their brain never suffered from dementia or other cognitive problems.
The failures also lend more significance to an “anatomical mismatch” that Alzheimer noted more than a hundred years ago: The two brain regions where the neural pathology of Alzheimer’s disease starts — the hippocampus and the nearby entorhinal cortex — generally show the least accumulation of amyloid plaques. Instead, amyloid plaques first get deposited in the frontal cortex, which gets involved in later stages of the disease and doesn’t show a lot of cell death, Small said. Decades can pass between the first appearance of amyloid and tau deposits and the neural death and cognitive decline seen in the disease — which raises questions about the causal connection between them.
The hypothesis took another hit last July when a bombshell article in Science revealed that data in the influential 2006 Nature paper linking amyloid plaques to cognitive symptoms of Alzheimer’s disease may have been fabricated. The connection claimed by the paper had convinced many researchers to keep pursuing amyloid theories at the time. For many of them, the new exposé created a “big dent” in the amyloid theory, Patira said.


Merrill Sherman/Quanta Magazine
Merrill Sherman/Quanta Magazine
Aisen acknowledges that science should encourage researchers to take different approaches. “But of course, in academic medicine and in commercial science, everybody has a lot riding on the outcome,” he said. “Careers are dependent upon the answer.”
And there was a lot riding on the amyloid hypothesis. It takes on average more than a decade and $5.7 billion to develop a single drug for Alzheimer’s disease. “Pharmaceutical companies are not shy in saying that they’ve invested many billions of dollars in this,” Nixon said.
Perhaps because of those heavy commitments and the near lock that the amyloid hypothesis had on public attention, some researchers faced pressure to accept it even after its unsuccessful track record was clear.
When Travaglini was a first-year graduate student at Stanford University in 2015, he was drawn to Alzheimer’s research as a focus for his doctoral thesis. It felt like a natural choice: His grandmother had been officially diagnosed with the disease, and he had already spent dozens of hours scouring the medical literature for information that might help her. He sought out the advice of two professors who were teaching a cell biology class he was taking.
“They were like, ‘Don’t even focus your class project on that,’” Travaglini said. They assured him that Alzheimer’s was basically already solved. “It’s going to be amyloid,” he remembers them saying. “There’s going to be anti-amyloid drugs that are going to work in the next two or three years. Don’t worry about it.”
Travaglini then went to a third professor who also told him to steer clear of Alzheimer’s, not because it was going to be solved but because “it’s just too complicated.” Tackle Parkinson’s instead, the professor said: Scientists had a much better sense of that disease, and it was a much simpler problem.
Travaglini shelved his plans to work on Alzheimer’s disease and instead did his thesis on mapping the lung.
Researchers who were already committed to non-amyloid approaches to Alzheimer’s say that they ran into a lot of resistance. There were many people who “suffered under the yoke of the amyloid people,” Small said. They couldn’t get grants or funding — and they were, in general, discouraged from pursuing the theories they really wanted to pursue.
“It was frustrating trying to get different stories out there,” Weaver said. It’s been “an uphill struggle” to get funding for his non-amyloid work.
When George Perry, a professor at the University of Texas, San Antonio put forth his theories that amyloid was coming from inside the neurons, “everybody hated it,” he said. “I discontinued the work because I couldn’t get funding for it.”
“There isn’t some great conspiracy or anything” to ban alternative approaches, said Rick Livesey, a professor of stem cell biology at University College London. But he notes that “there are some issues around innovation in dementia research.”
In 2016, Christian Behl, a professor of biochemistry at the University Medical Center of the Johannes Gutenberg University of Mainz in Germany, took the bold step of organizing a meeting called “Beyond Amyloid,” an open-ended discussion of new ideas about the causes of Alzheimer’s disease. “I personally got quite some criticism from different colleagues out of the amyloid fields that disliked the idea to do such a meeting,” he said.
Enlarged Endosomes
Despite the obstacles, some non-amyloid-cascade research did make landmark progress during the early 2000s. In particular, a critical finding around the turn of the millennium reinvigorated interest in the lysosomal explanation.
Anne Cataldo, a postdoctoral fellow in Nixon’s lab, was studying the properties of organelles called endosomes in Harvard’s donated brains. Endosomes are a highly dynamic network of vesicles that sit under the cell membrane and aid lysosomes. Their job is to take in proteins and other materials from outside the cell, sort them, and ship them where they need to go — sometimes to the lysosomes for autophagy. (Think of endosomes as a cell’s version of FedEx, said Young.)
Cataldo noticed that in the brains from Alzheimer’s patients, the endosomes in neurons were abnormally large, as though the endosomes were struggling to process the proteins they were picking up. If molecules slated for destruction don’t get labeled, recycled or shipped properly, that disruption of the endosomal-lysosomal pathway can trigger a cascade of problems both inside and outside cells. (Imagine unsorted, undelivered packages piling up in the fleet of FedEx trucks.)
The endosome enlargement might have seemed like just a consequence of the increasing brain pathology except for two important points: It didn’t happen in the brains of people with other neurodegenerative diseases that they examined, only Alzheimer’s. And the enlargement started happening before amyloid plaques were deposited.
“That finding was very pivotal,” Nixon said.
Furthermore, Cataldo showed that the endosomes were enlarged in people who did not yet have symptoms of Alzheimer’s but who carried a mutation, APOE4, that affected how their body handles cholesterol. APOE4 is the most significant genetic risk factor ever found for late-onset Alzheimer’s. (It’s the mutation that the actor Chris Hemsworth, famous as the movie superhero Thor, recently learned that he carries.) People who have one copy of APOE4 have a two- to threefold elevated risk of developing Alzheimer’s; people like Hemsworth who have two copies have an eight-to twelvefold elevated risk.
Cataldo, Nixon and their colleagues published their findings in 2000. Since then, evidence has implicated lysosomal disruptions in problems ranging from neurodegenerative diseases to “lysosomal storage diseases,” in which toxic molecules pile up in lysosomes instead of breaking down. It was also discovered that when APP is cleaved to make amyloid-beta in neurons, it happens inside their endosomes. And studies have shown that the endosomal-lysosomal system routinely starts to slow down and malfunction in aging cells — a fact that has made these organelles into hot topics for longevity research.
Nixon suspects that the endosomal-lysosomal pathway, the amyloid cascades, neuroinflammation and other processes all contribute to Alzheimer’s as elements of a disease model that he sometimes calls “the elephant.”
Karen Dias for Quanta Magazine
Cataldo died in 2009, and work on endosomes in Nixon’s lab and with his collaborators stalled. But Small and his team were knee-deep in this research area at the time. In 2005, they found evidence that in certain endosomes, a complex of proteins known as a retromer might be malfunctioning in Alzheimer’s disease and triggering endosomal traffic jams that cause amyloid to accumulate in neurons.
The Persuasive Power of Genetics
Just as the genetics experiments in Hardy’s lab and others first helped propel the amyloid cascade hypothesis to prominence, genetics did something similar for the alternative hypotheses over the past 15 years. “Genetics is definitely seen as the anchor for people to try and make sense of stuff,” Livesey said.
Starting in 2007, massive statistical studies of the genome identified dozens of new genetic risks for Alzheimer’s. These genes were generally far weaker in their effects than APOE4, but they all increased the likelihood that someone might develop Alzheimer’s. They also directly connected the late-onset forms of the disease to multiple biochemical pathways in cells, including the immune system, cholesterol metabolism and the endosomal-lysosomal system. Many of these genes were also among the earliest to become active in Alzheimer’s disease. These discoveries were when others started to believe “this is meaningful,” Nixon said.
The endosomal-lysosomal hypothesis was not only becoming more concrete; it was looking increasingly likely to be an essential piece of the Alzheimer’s puzzle.
Supporters of the amyloid cascade hypothesis, however, still believe the genetics are on their side. The only three genes known to directly cause Alzheimer’s, rather than just increasing the risk for it, are for the proteins APP (the bane of the Jennings family), presenilin 1 and presenilin 2 — and mutations in all three of them cause pileups of amyloid.
“Anybody who looks at that and says amyloid is not causative is just either hiding their head in the ground, or they’re being disingenuous,” Tanzi said. “Genetics will set you free.”
But studies have also suggested that those genes could be involved in ways that don’t depend on the amyloid hypothesis. For example, in 2010, Nixon and his team reported that mutations in presenilin 1 disrupted lysosomal function. Evidence also suggested that all three causal genes are involved in making endosomes swell.
The debates about what the findings mean are still fierce, but many researchers in the Alzheimer’s field are feeling a rumbling beneath their feet as the field shifts toward the idea that “amyloid is not unimportant, but it’s not the only thing,” Nixon said. “Now there’s a sufficient number of people [on board] that I think the message is, ‘Do your own thing now.’”
Flowers of Dementia
On Nixon’s desk is a copy of the June issue of Nature Neuroscience, and next to it a mug that has the issue’s cover printed on it, given to him by the lead author of the study.
In the cover feature of that issue, Nixon and his team reported one of the most powerful pieces of evidence yet that the simple version of the amyloid hypothesis is wrong and that something deeper within neurons is fundamentally malfunctioning. If their findings in mice and a handful of human tissues hold true in follow-up studies, they could critically change our understanding of the origins of Alzheimer’s disease.
Using a novel probe, they fluorescently labeled lysosomes involved in autophagy in mice that had been genetically induced to develop Alzheimer’s disease. The probe allowed the researchers to watch the disease progress in living mice under a giant confocal microscope. The first of the resulting micrographs was “the most spectacular image that we’ve ever collected,” Nixon said. “It was so out of the realm of anything I had seen.” It showed structures in the brain that looked like flowers.
These “flowers” turned out to be neurons bulging with toxic accumulations of proteins and molecules. After a contest among the team members, the team decided to name these neurons “PANTHOS,” from the ancient Greek word for flower (ánthos) with an added “p” for poison.
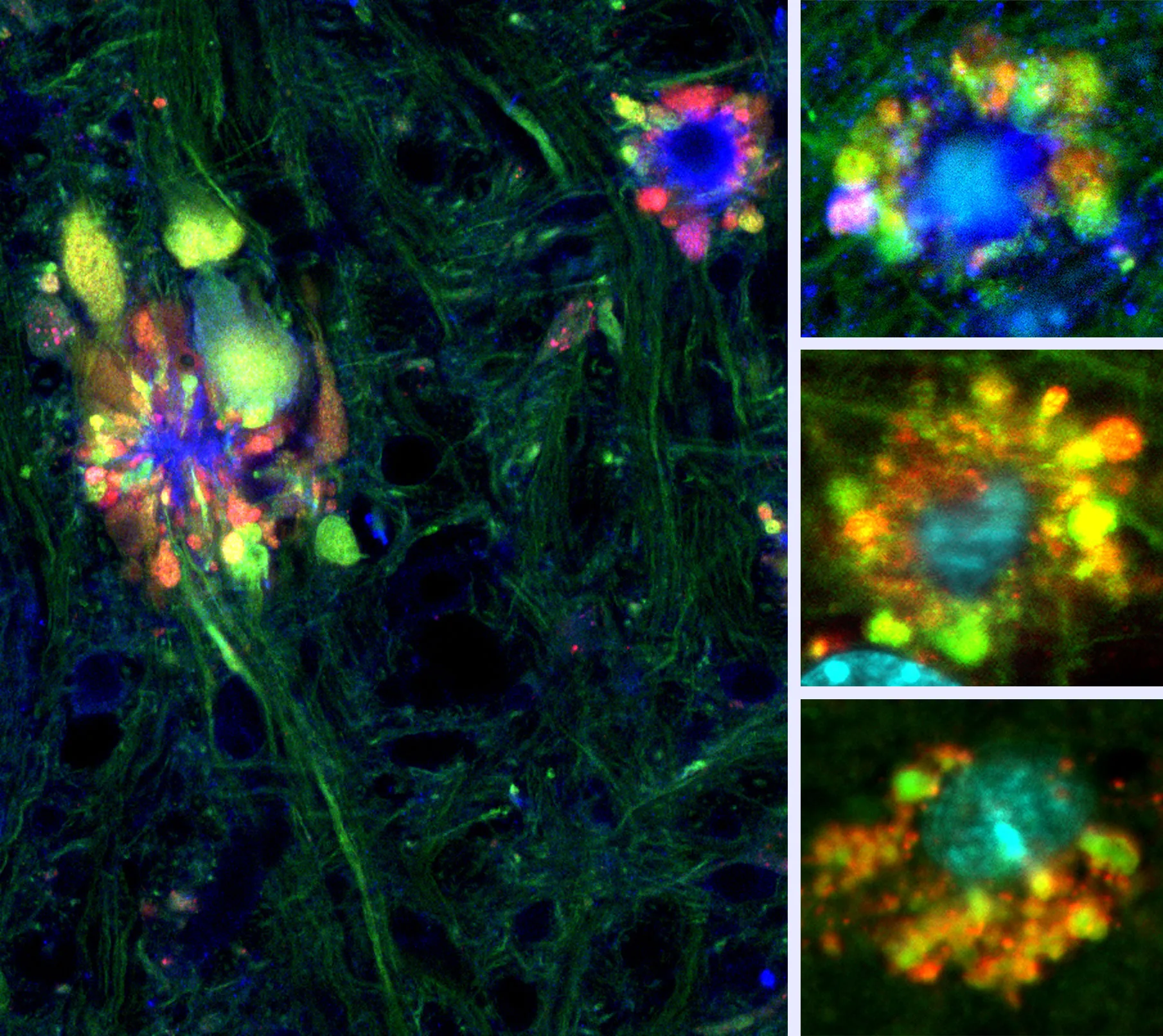
Nixon and his group discovered that lysosomal dysfunctions can cause diseased neurons to erupt into structures they called PANTHOS. In micrographs, PANTHOS neurons look astonishingly like flowers, but they are dying cells.
Ju-hyun Lee
Further work revealed that the PANTHOS neurons were products of autophagy gone wrong. Normally in autophagy, highly acidic lysosomes carrying digestive enzymes fuse with vesicles carrying waste. The fusion results in a structure known as an autolysosome, in which the waste is digested and then recycled into the cell. In mice with Alzheimer’s, however, the autolysosomes were swelling with accumulations of amyloid-beta and other waste proteins. The lysosomes and autolysosomes were not acidic enough for the enzymes to digest the waste.
The neurons kept making more and more autolysosomes, each of which grew bigger and bigger. Soon they were poking into the cell membrane, pushing it outward to form the “petals” of the flower shapes that Nixon had seen. Engorged autolysosomes also accumulated in the center of the neuron, fusing with the organelles there and forming piles of amyloid fibrils that started to look like plaques.
Eventually, the autolysosomes burst and released their toxic enzymes, damaging and slowly killing the cell. The dead cell’s contents then leaked into the surrounding space — and started poisoning nearby cells, which in turn also became PANTHOS neurons before exploding. Microglia, cells that are part of the brain’s immune system, swooped in to clean up the mess, but in the process they also started damaging nearby neurons.
Nixon and his co-workers also realized something else: With traditional staining and imaging methods, the masses of proteins accumulating in the autolysosomes inside PANTHOS neurons would have looked exactly like classic amyloid plaques outside of cells. The extracellular amyloid plaques weren’t killing the cells — because the cells were already dead.
Their discovery implied that anti-amyloid therapies would be futile. “It’s like trying to cure a disease in someone who’s buried in the cemetery,” Nixon said. “Removing the plaque is removing the tombstone.”
Because their initial findings were in mice, the team searched for similar PANTHOS neurons in human samples. Knowing what to look for, they found them easily. Sitting at the controls of the confocal microscope that filled half of a dark and dusty room in Nixon’s lab, the research scientist Philip Stavrides toggled the field of focus up and down over one of the human Alzheimer’s brain samples. Bright bursts of the greens, reds and blues of the poisonous “flowers” filled the microscope’s screen.


Merrill Sherman/Quanta Magazine
“It is really a very interesting paper, and a step closer to the cause,” said Charlotte Teunissen, a professor of neurochemistry at the Amsterdam University Medical Centers. Understanding the mechanisms of early disruptions in Alzheimer’s disease could help not only in developing drugs, but also in identifying biomarkers, she added. The paper “was exceptional,” said Perry.
People have long debated which form of amyloid is most toxic and where it does the most damage, and this study provided ample evidence that intracellular amyloid may play an important role in the disease, Aisen said. What could be interesting now, he said, would be for neuropathologists to check how frequently and extensively these abnormalities appear in Alzheimer’s brains. For drug therapy research, he thinks there’s now “all the more reason to continue exploring small molecules that can penetrate into the cell and actually inhibit the enzymes that generate the amyloid-beta.”
Since the PANTHOS paper was published, Nixon and his team may have discovered why the lysosomes in Alzheimer’s patients are not acidifying properly. When APP is being digested in the endosome, one of the byproducts is amyloid-beta, but another one is a protein called beta-CTF. Too much beta-CTF inhibits the lysosome’s acidification system. Beta-CTF could therefore be another important potential target for drug development that has generally been ignored, Nixon said.
All the Parts of the Elephant
A week after he published the PANTHOS paper, Nixon and several other researchers were awarded the Oskar Fischer Prize, an award given at the University of Texas, San Antonio for novel ideas that gaze beyond prevailing theories of Alzheimer’s disease.
The award was originally intended to be for the one person who came up with the most comprehensive explanation of the causes of Alzheimer’s disease. But the founders eventually broke it up into multiple prizes “because it’s impossible to capture every different aspect” of such a complex disease, Nixon said.
Nixon won for his description of problems in the ability of endosomes to traffic proteins and lysosomes to clear proteins. Others won for their work on abnormalities in cholesterol metabolism, mitochondria, neural stem cells and neuron identities.
The hypothesized sequence of events in the pathology is murky; various arguments can be made for what comes first, second or third. But all the dysfunctional pathways — involving the endosomes and lysosomes, the immune system, cholesterol metabolism, mitochondria, neural stem cells and the rest — might be intertwined pieces of a single gigantic puzzle.
“They, in my mind, can all be integrated into one entity, which I call the elephant,” Nixon said. Endosomal-lysosomal dysfunctions, for example, could easily influence all the other pathways and send disruptions rippling throughout individual cells and the brain. But if the dysfunctions are intertwined, there might not be a single definitive trigger for Alzheimer’s disease.
Other researchers are also beginning to see Alzheimer’s disease less as a single discrete disorder than as an assortment of processes that go wrong together. If that’s true, treatments that target just one protein in this cascade, such as amyloid, might not have much of a therapeutic benefit. But a cocktail of drugs — say, one that targets the elephant’s legs, one that targets its tail and one that targets its trunk — might be enough to knock the animal down.

Nixon hopes to uncover the proteins other than amyloid that play a major role in endosomal-lysosomal dysfunction.
Karen Dias for Quanta Magazine
Still, too many people insist on casting the debate over what causes Alzheimer’s as an either-or problem, Nixon said. They chide him, arguing that his beliefs about the importance of the endosomal-lysosomal mechanism must mean that he doesn’t believe amyloid-beta has any role in the disease. “It’s like you can’t hold two relevant ideas in juxtaposition,” he said.
In Alzheimer’s disease, amyloid-beta may be one killer, but there could be a range of toxic accumulating proteins that are equally important in killing the cell, he said. Amyloid-beta is like a banana peel in a garbage can. “There’s a whole host of other garbage that might be even more disgusting than the banana peel,” Nixon said.
Small agrees that it could make the most sense for the endosomal-lysosomal hypothesis, the neuroinflammation hypothesis and the amyloid cascade hypothesis to combine at some point into one larger theory. “You can Occam’s-razor this,” he said.
The implications of taking this broader perspective could reach beyond the Alzheimer’s field. Clues gleaned from Alzheimer’s could help our understanding of other neurodegenerative disorders, such as Parkinson’s disease and amyotrophic lateral sclerosis (ALS, or Lou Gehrig’s disease) — and aging. The reverse could also apply: Weaver often reads the ALS and Parkinson’s literature as well, hoping that their insights “will flip over to our world,” he said.
New Drugs, New Theories
Enthusiasm for explanations beyond the amyloid cascade hypothesis doesn’t mean that people have lost interest in the anti-amyloid drugs now being tested. Aisen and many other researchers are still optimistic that we can build on the moderate success of lecanemab. Even if the drugs address only part of what’s wrong in Alzheimer’s disease, any improvement could be a lifeline for patients.
“Patients need something,” Weaver said. “And I really hope that one of these [ideas] turns out to be right.”
After so many years of drug failures, the lecanemab results were welcome news for Hardy. He flew from London to San Francisco so he could be present when the results were presented at the end of November at the Clinical Trials on Alzheimer’s Disease conference. He could have watched the results from home online, but he wanted to be part of the excitement and “to hear what other people think of the results.”
Even though Hardy helped to launch the amyloid cascade hypothesis decades ago and still believes in its power, he has also always been extremely receptive to evolving ideas.
In 2013, Hardy and his team discovered that mutations in a gene involved in the immune system could increase the risk of developing late-onset Alzheimer’s disease. Since then, he has shifted the focus of his lab to studying microglia. He suspects that amyloid deposits might activate microglia directly to cause damaging inflammation.
To many researchers, the immune system offers an appealingly flexible explanation for Alzheimer’s, one that fits with both the amyloid hypothesis and other ideas. A report in the July 2020 issue of The Lancet listed the variety of known risk factors for dementia, ranging from air pollution to repetitive head trauma to systemic infections. “I mean, it goes on and on,” Weaver said. “They’re different as night and day.”
The thread that connects them, he continued, is the immune system. If you bang your head and damage tissues, the immune system steps in to clean up the mess; if you get infected by a virus, your immune system wakes up to fight it; air pollution activates the immune system and causes inflammation. Studies have shown that even social isolation can lead to inflammation of the brain, and depression is a known risk factor for dementia, Weaver said.
The immune system is also intimately connected to the lysosomal system. “How cells use the lysosomal pathway to internalize, degrade or recycle proteins is critical to how a neuroimmune response may occur,” Young said.
But the endosomal-lysosomal network is also very finely tuned and has a multitude of moving parts that work differently in different types of cells. That makes it trickier to target, Young said. Still, she’s hopeful that there will be a burst of new clinical trials targeting this network in the next few years. Young, Small and Nixon are all working on targeting different aspects of this network.
Part of the allure of the amyloid cascade hypothesis was that it offered a simple solution to Alzheimer’s disease. Some of these other hypotheses bring in extra layers of complexity, but it’s a complexity that scientists — and a growing number of startups — now seem willing to tackle.
Waiting for Relief
Travaglini went back to Alzheimer’s research at a late stage of his doctoral work. In October 2021, he started at the Allen Institute, sifting through slices of brain samples from people who had died of the disease. He and his team are compiling the Seattle Alzheimer’s Disease Cell Atlas — a reference that will detail the effects of the disease on the brain’s diverse mix of cells. As part of that work, they are analyzing changes in the activity of more than a hundred kinds of cells in the cortex during the progression of Alzheimer’s disease.
“The cellular face of the disease is so important, because it puts all of these molecular changes and hypotheses into the context of the cell that they’re actually occurring in,” Travaglini said. If you put amyloid or tau protein on cells in a dish, the cells start to deteriorate and die. “But it’s not been so clear how different kinds of cells are changing.”
His work has already turned up interesting insights, such as the fact that the neurons most vulnerable to the disease are those that have made extra-long connections across the cortex of the brain — where much of our cognitive ability arises. Something about that type of cell could make it more susceptible to the disease, he said.
Travaglini and his co-workers have also seen an increase in the number of cells such as microglia, adding even more evidence to the idea that neuroinflammation is a major part of the process. They have also already uncovered a number of genes that are expressed improperly in the brains of people with Alzheimer’s disease, including genes linked to the lysosomal-endosomal network. Eventually, their work could help to uncover the timing of when things go wrong in specific cells, teasing apart one of the greatest mysteries of the disease.

Kyle Travaglini, his brother Colin, his grandmother and his grandfather.
Courtesy of Kyle Travaglini
Travaglini has tried to visit his grandparents as often as possible. A while ago, his grandmother needed to be moved into an assisted-living memory home; his grandfather went too. “He wanted to be with her,” Travaglini said.
They were constant companions since they met in Philadelphia in college; they married more than 60 years ago in Japan, where he was stationed for military service. It has always been hard on him to see her slip away, but it became even harder recently when he too was diagnosed with dementia, although not Alzheimer’s. He would speak lovingly of her, but then add “she doesn’t really like me anymore,” Travaglini said. The family would remind him that wasn’t true, that it was the disease.
Early in the morning of December 1, Travaglini’s grandmother died. She was 91.
Her Alzheimer’s had progressed too far for her to understand what her grandson was working on, but his grandfather at least had a chance to know that Travaglini pursued research in the dementia fields. “He was really proud of that,” Travaglini said.
Family support matters to researchers like Travaglini in more ways than one. Millions of families are volunteering to help test new drugs and new ideas to advance understanding of Alzheimer’s disease, knowing full well that the results likely won’t materialize soon enough to help them.
Until effective treatments are found, Patira will continue to treat the dementia patients in her care by holding their hands through the journey and helping them navigate their evolving relationships with their families. Her patients’ biggest fear is that they will no longer be able to recognize their grandchildren. “That’s painful to think for yourself,” she said. “And that’s painful to think for the loved ones.”
Research in the field, now more open to other alternatives, will continue to move along, with both good and bad news. “Even if the studies don’t work, you learn something from the failures,” Patira said. “It’s frustrating as a clinician, but it’s good for science.”
‘Carol Knew the Implications’
Shortly after Hardy’s discovery that the APP gene was why her family was so afflicted with Alzheimer’s, Carol Jennings quit her job as a teacher to work full-time supporting and advocating for Alzheimer’s disease research. In the following decades, she worked closely with Hardy and then with other researchers at University College London.
Jennings never took the genetic test for the APP mutation that led to her father, three aunts and an uncle — five out of the 11 people in her family — developing Alzheimer’s disease. “She didn’t think it was worthwhile, because there was nothing that we could do,” said Stuart Jennings, Carol’s husband, who is a Methodist minister and historian. “She would say, ‘I could get run over by a bus tomorrow; why worry about something that’s going to happen in 30 years’ time?’” Their two children have likewise not been tested.
In 2012, Carol Jennings was diagnosed with Alzheimer’s disease. She was 58 years old.
Carol Jennings is one of the very small fraction of people whom researchers can look at and say exactly why her brain has deteriorated. The brains of the vast majority of Alzheimer’s patients, whose disease isn’t tied to a specific gene, are more open to interpretation.
“The interesting thing is that the early symptoms were [that] the things that she did badly got worse,” Stuart Jennings said. “We all used to joke she could get lost going from the bedroom to the bathroom.” Eventually, that became literally true. She had always procrastinated, but she became very last-minute.
Then the things she was good at, like packing and organizing, started to deteriorate. It took years for her to get a formal diagnosis, but once she did, it was traumatic for the first couple of days, Stuart said: “Carol knew what the implications were.”
So she started giving instructions. When she dies, she told Stuart, her brain must be donated to the brain bank run by the team at University College London, as the brains of her other afflicted family members have been. She told him that he didn’t have to keep her at home if he couldn’t cope, but he must keep her clean. All the little details were ironed out. “She was brilliant. She got it all organized. I just supported her, really,” Stuart said.
He has managed to keep her at home, and UCL researchers continue to follow the Jennings family. Carol and Stuart’s son John works closely with them now, too.
As he spoke over Zoom, Stuart sometimes patted Carol’s head from his seat beside her, as she lay in bed with a cold. Because of her Alzheimer’s, she can’t get out of bed or talk anymore other than to give yes or no answers to certain prompts. During the conversation, she drifted in and out of sleep — but when she was awake and watching the interview, it didn’t feel as though she was silent.
Maybe in those moments some part of her was back onstage lecturing about Alzheimer’s disease, stringing words together with ease, inspiring and awing an audience. In her talks, she would stress the idea that “this is about families, not about test tubes and labs,” Stuart said. “That was quite powerful, I think, for the drug reps to hear.”
Carol wasn’t bothered that disease-altering treatments didn’t arrive in time to help her — to her, that was a small point. “Carol’s always worked on the principle that it’s for the children and for the next generations,” Stuart said.

Correction: December 8, 2022
This article initially credited the wrong photographer for the photos of Ralph Nixon. Those photos were taken by Karen Dias for Quanta Magazine.



